


Gene therapy for thalassemia delivers corrected genetic material into a patient’s stem cells to restore healthy hemoglobin production. Approved treatments like betibeglogene spartacus (Zynteglo) have shown transfusion independence in clinical trials, representing a potential one-time cure. Cost, access, and long-term safety remain key challenges.
Thalassemia affects more than 300 million people worldwide, according to the Thalassemia International Federation. For decades, patients with beta thalassemia major have relied on lifelong blood transfusions and iron chelation therapy just to survive. These treatments carry serious burdens—physical, emotional, and financial—and they manage the disease rather than cure it.
Gene therapy for thalassemia changes that equation fundamentally. Rather than compensating for a genetic defect, thalassemia gene treatment targets the root cause: the faulty or missing instructions that prevent the body from producing healthy hemoglobin. The result, in the most successful cases, is a patient who no longer needs regular transfusions at all.
This guide covers everything you need to know—how gene therapy works, what the science actually involves, which treatments have reached approval, what challenges remain, and what the future of advanced thalassemia treatment options looks like. Whether you are a patient, caregiver, or clinician, the goal here is clarity: no unnecessary jargon, no false promises, just an honest account of where the field stands today and where it is heading.
What Is Thalassemia and Why Do Current Treatments Fall Short?
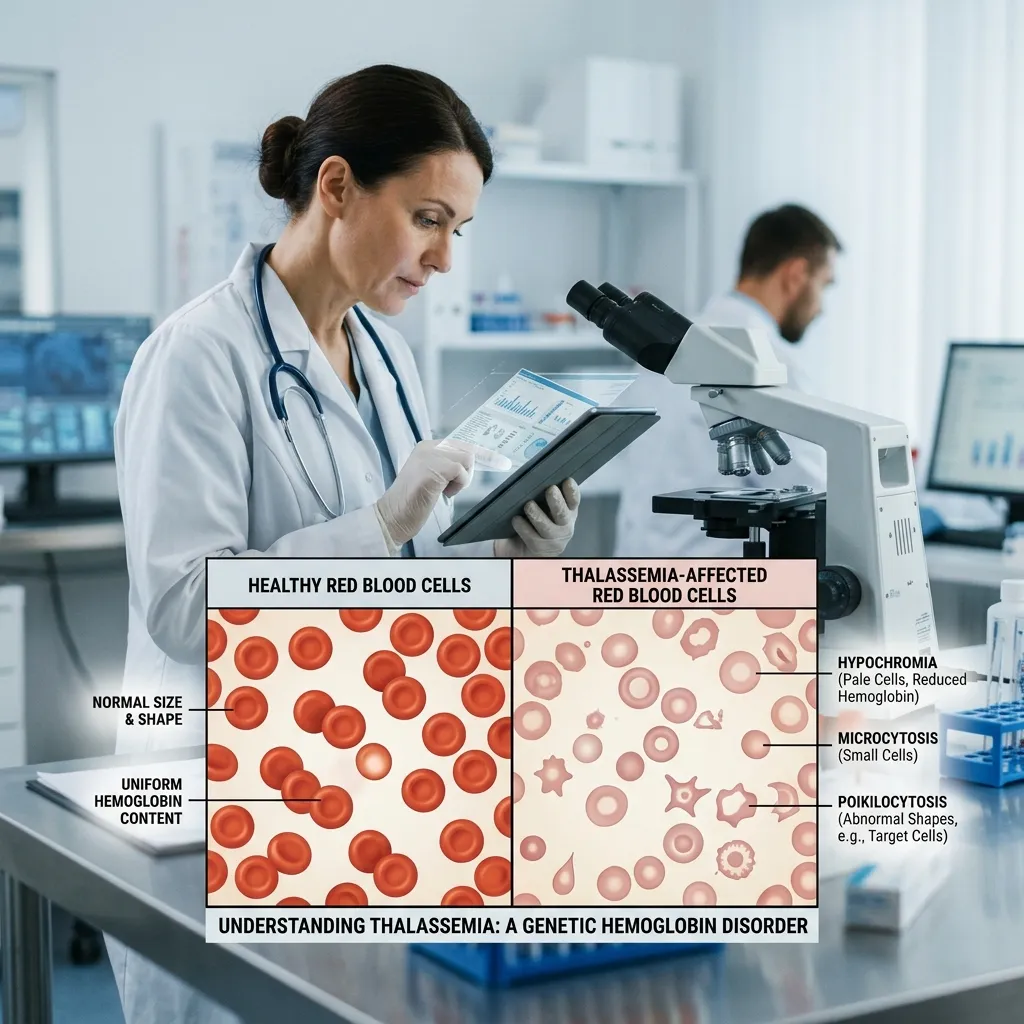 Thalassemia is an inherited blood disorder caused by mutations in the genes responsible for producing hemoglobin—the protein inside red blood cells that carries oxygen throughout the body. When these genes malfunction, the body produces too few healthy red blood cells, leading to anemia that ranges from mild to life-threatening.
Thalassemia is an inherited blood disorder caused by mutations in the genes responsible for producing hemoglobin—the protein inside red blood cells that carries oxygen throughout the body. When these genes malfunction, the body produces too few healthy red blood cells, leading to anemia that ranges from mild to life-threatening.
Beta thalassemia major, the most severe form, requires blood transfusions every two to four weeks. Each transfusion temporarily restores hemoglobin levels, but repeated transfusions accumulate iron in the organs. Without chelation therapy to remove that excess iron, patients face damage to the heart, liver, and endocrine system. Even with optimal management, the treatment burden is relentless—frequent hospital visits, daily medications, and constant monitoring. For a deeper look at how this chronic burden affects mental health, the guide on the psychological impact of thalassemia outlines the emotional toll in detail.
Bone marrow transplantation offers a potential cure, but it requires a matched donor, carries significant risks of graft-versus-host disease, and is unavailable to most patients globally. That gap—between what conventional treatment can offer and what patients actually need—is exactly where genetic therapy for beta thalassemia enters.
How Does Gene Therapy for Thalassemia Work?
What Is the Basic Mechanism of Thalassemia Gene Treatment?
Gene therapy for thalassemia works by introducing a functional copy of the beta-globin gene into a patient’s own stem cells. Once those corrected stem cells are reinfused into the patient’s bloodstream, they take up residence in the bone marrow and begin producing healthy hemoglobin on their own.
The process, simplified, follows these steps:
- Stem cells are collected from the patient’s blood or bone marrow.
- A viral vector—engineered to carry the corrected gene—delivers the functional gene into those stem cells in the laboratory.
- The patient undergoes conditioning chemotherapy to clear space in the bone marrow.
- The corrected stem cells are reinfused and begin producing healthy red blood cells.
Because the corrected cells are the patient’s own, the risk of rejection is substantially lower than with a donor transplant. This autologous approach is one of the most significant advantages of modern gene therapy for thalassemia.
What Are the Main Types of Gene Therapy Approaches for Blood Disorders?
Two primary strategies are used in genetic therapy for beta thalassemia today:
Lentiviral gene addition inserts a functional beta-globin gene into the patient’s stem cells using a modified lentiviral vector. Betibeglogene spartacus (Zynteglo), approved by the FDA in 2022 and the EMA in 2019, uses this approach. Clinical trial data showed that the majority of patients with beta thalassemia major treated with Zynteglo achieved transfusion independence.
Gene editing with CRISPR-Cas9 takes a different approach. Rather than adding a new gene, CRISPR-based therapies reactivate the patient’s fetal hemoglobin (HbF)—a form of hemoglobin produced before birth that can compensate for defective adult hemoglobin. Exagamglogene autotemcel (Casgevy), approved by the FDA in December 2023, became the first CRISPR-based therapy approved for any disease. It targets BCL11A, a gene that suppresses fetal hemoglobin production, effectively switching fetal hemoglobin back on.
What Role Do Viral Vectors Play in Delivering Gene Therapy?
Viral vectors are the delivery vehicles of gene therapy. For thalassemia gene treatment, lentiviral vectors are most commonly used because they can integrate their genetic payload into the host cell’s DNA in a stable, long-lasting way.
Safety modifications are built into therapeutic vectors to prevent them from replicating or causing disease on their own. Decades of research have refined these tools considerably, though the risk of insertional mutagenesis—where the inserted gene disrupts a nearby gene—remains a subject of ongoing monitoring.
The Clinical Journey: Trials, Milestones, and Approvals

What Have Clinical Trials Revealed About Gene Therapy for Thalassemia?
The HGB-207 and HGB-212 clinical trials for Zynteglo, published in the New England Journal of Medicine and presented at major hematology conferences, demonstrated that approximately 89% of participants with non-severe beta thalassemia genotypes achieved transfusion independence. Among the broader trial population, the majority saw significant reductions in transfusion requirements.
The CLIMB THAL-111 trial for Casgevy reported that 39 of 42 evaluable participants with transfusion-dependent beta thalassemia were free from transfusions during a continuous 12-month period, according to data presented at the American Society of Hematology annual meeting in 2023.
These are not incremental improvements. They represent transformational outcomes for a patient population that previously had no path to treatment independence outside of a matched donor transplant.
What Does FDA and EMA Approval Mean for Thalassemia Patients?
The FDA approval of Zynteglo in August 2022 marked the first gene therapy approval in the United States for beta thalassemia. The EMA had approved the same therapy in 2019. The FDA approval of Casgevy in December 2023 added a second approved option, this time using CRISPR technology.
Regulatory approval means that these therapies have met rigorous standards for safety and efficacy. For patients and families, it signals that advanced thalassemia treatment options have moved from experimental to clinical reality. For healthcare systems, it raises urgent questions about access, cost, and implementation.
Benefits of Gene Therapy: What Patients Stand to Gain
Can Gene Therapy Offer a One-Time Cure for Thalassemia?
The word “cure” is used cautiously in medicine, but the goal of gene therapy for thalassemia is to deliver a single, permanent intervention that eliminates the need for ongoing transfusions. If corrected stem cells engraft successfully and continue producing healthy hemoglobin over the long term, the therapeutic benefit is potentially lifelong.
Long-term follow-up data are still accumulating—the field is too young to claim decades of evidence—but results at the five- and seven-year marks for early gene therapy recipients remain encouraging, with most participants maintaining transfusion independence.
How Does Thalassemia Gene Treatment Improve Quality of Life?
The quality-of-life gains from successful thalassemia gene treatment are substantial. Patients freed from regular transfusions regain time—time previously spent at infusion centers, recovering from procedures, or managing medication schedules. Iron overload, a major driver of organ damage and emotional distress, stops accumulating. The constant anxiety of managing a chronic, life-threatening condition decreases. For many patients, the emotional wellbeing benefits are as significant as the physical ones. Understanding how to manage the emotional dimensions of thalassemia care remains important even as physical treatment advances; resources on emotional wellbeing in thalassemia care can help patients and families navigate that transition.
Challenges and Considerations in Gene Therapy for Thalassemia

What Are the Safety Risks Associated With Thalassemia Gene Treatment?
No medical intervention is without risk, and gene therapy for thalassemia is no exception. The most significant concerns include:
- Insertional mutagenesis: The risk that a lentiviral vector integrates into a location that disrupts normal gene function. Careful vector design and long-term monitoring address this risk.
- Conditioning chemotherapy: Patients must undergo myeloablative chemotherapy before receiving corrected cells. This clears the bone marrow but carries its own short-term risks, including infection, infertility, and fatigue.
- Off-target gene editing: CRISPR-based therapies carry a theoretical risk of editing unintended areas of the genome. Current data suggest this risk is low, but monitoring continues.
- Engraftment failure: In rare cases, corrected stem cells may not successfully establish themselves in the bone marrow.
How Accessible and Affordable Is Gene Therapy for Thalassemia Today?
This is where the promise of gene therapy collides with hard reality. Zynteglo carries a list price of approximately $2.8 million per treatment in the United States, making it one of the most expensive therapies ever approved. Casgevy has a similar price range.
These costs reflect the complexity of manufacturing individualized treatments, years of research investment, and the expectation that a one-time therapy will offset decades of transfusion costs. Whether insurance systems and healthcare payers accept that logic varies enormously by country and plan.
For most thalassemia patients globally—many of whom live in low- and middle-income countries where the disease burden is highest—these treatments remain out of reach. Global access is the defining ethical challenge of the gene therapy era.
What Ethical Questions Does Genetic Therapy for Beta Thalassemia Raise?
Germline editing—making changes that would be inherited by future generations—remains prohibited in clinical applications. Current approved therapies modify only somatic cells (the patient’s own stem cells), so genetic changes are not passed on. But as gene editing technology becomes more powerful and precise, debates about the boundaries of intervention will intensify.
Questions of equity, consent in pediatric patients, and the commercialization of curative therapies are all active areas of discussion in bioethics and health policy. These conversations are as important as the science itself.
Advanced Thalassemia Treatment Options Beyond Gene Therapy
What Other Emerging Therapies Are Showing Promise?
Gene therapy for thalassemia does not exist in isolation. Several other advanced thalassemia treatment options are in various stages of development:
- Luspatercept (Reblozyl): An FDA-approved erythroid maturation agent that reduces transfusion burden in adults with beta thalassemia. It does not cure the disease but reduces the frequency of transfusions needed.
- Fetal hemoglobin inducers: Drugs that reactivate fetal hemoglobin production through non-CRISPR mechanisms are under investigation as potentially more accessible alternatives.
- Next-generation gene editing tools: Base editing and prime editing—more precise successors to standard CRISPR-Cas9—are being explored in preclinical and early clinical work, with the potential to correct mutations without making double-strand DNA breaks.
How Do Combination Therapies Fit Into the Future of Thalassemia Care?
For patients who are not candidates for gene therapy—due to age, health status, or access limitations—combination approaches that pair luspatercept with optimized iron chelation or other supportive agents may significantly reduce treatment burden even without achieving transfusion independence.
Thalassemia care is becoming increasingly individualized. Comprehensive, patient-centered approaches that account for disease severity, genetic subtype, lifestyle, and treatment goals are replacing the one-size-fits-all transfusion model. For more on how holistic care models are being applied in practice, the holistic thalassemia care plans resource provides a useful framework.
Patient Perspectives and Real-World Impact

What Do Patient Outcomes Tell Us About Gene Therapy for Thalassemia?
Clinical trial data capture outcomes, but they cannot fully convey what transfusion independence means to a patient who has spent years organizing their life around infusion schedules. Published accounts and patient advocacy reports describe profound shifts—in confidence, in life planning, in relationships—for those who have successfully undergone thalassemia gene treatment.
Patient advocacy organizations, including the Thalassemia International Federation, have been instrumental in pushing for faster regulatory review, more transparent pricing negotiations, and expanded access programs. Their work connects scientific progress to the people who most need it.
How Should Gene Therapy Be Integrated Into Existing Thalassemia Care Models?
Gene therapy does not eliminate the need for ongoing care—it transforms it. Post-treatment patients still require monitoring for engraftment success, iron levels, organ function, and long-term vector safety. Integrating genetic therapy for beta thalassemia into existing care pathways requires coordination between hematologists, genetic counselors, mental health professionals, and primary care providers.
Patients transitioning from transfusion-dependent care to post-gene therapy monitoring need structured follow-up protocols. Understanding long-term blood monitoring remains relevant even after successful treatment, because ongoing vigilance protects the gains that treatment achieves.
Conclusion:
Gene therapy for thalassemia represents a groundbreaking shift in how this lifelong blood disorder may be treated in the future. Unlike traditional treatments that focus on managing symptoms, gene-based approaches aim to correct the underlying genetic defect, offering the possibility of long-term or even permanent relief. Advances such as viral vector gene addition and CRISPR-based editing have shown promising results in clinical trials, bringing new hope to patients with severe beta-thalassemia.
However, challenges remain, including high treatment costs, limited accessibility, long-term safety concerns, and the need for specialized medical centers. While not yet widely available, ongoing research and regulatory approvals continue to move the field forward. As science progresses, gene therapy may become a transformative option that significantly improves quality of life and reduces the global burden of thalassemia.
Frequently Asked Questions About Gene Therapy for Thalassemia
1. What is gene therapy for thalassemia, and how does it differ from a blood transfusion?
Gene therapy for thalassemia targets the underlying genetic cause of the disease by inserting a functional beta-globin gene—or reactivating fetal hemoglobin—into the patient’s own stem cells. Blood transfusions replace deficient red blood cells temporarily but do not address the genetic defect. Gene therapy aims for a permanent correction rather than ongoing symptom management.
2. Which gene therapies for thalassemia have been approved by the FDA?
Two therapies are currently FDA-approved: betibeglogene spartacus (Zynteglo), approved in August 2022, and exagamglogene autotemcel (Casgevy), approved in December 2023. Casgevy is the first approved CRISPR-based gene therapy for any disease.
3. Who is eligible for gene therapy for thalassemia?
Current approvals cover patients aged 12 and older with transfusion-dependent beta thalassemia who do not have a matched sibling bone marrow donor. Eligibility also depends on overall health, organ function, and the ability to tolerate conditioning chemotherapy. Physicians evaluate candidates individually.
4. Is genetic therapy for beta thalassemia a permanent cure?
The goal is permanent correction. Clinical trial data show that most successfully treated patients remain transfusion-independent at five or more years of follow-up. However, “permanent” requires longer-term evidence than currently exists. Ongoing monitoring continues for all treated patients.
5. What are the main risks of thalassemia gene treatment?
Key risks include insertional mutagenesis from lentiviral vectors, side effects from conditioning chemotherapy (including infection risk and infertility), off-target editing effects in CRISPR-based therapies, and the possibility of incomplete engraftment. These risks are considered manageable with proper selection, treatment, and follow-up protocols.
6. How much does gene therapy for thalassemia cost, and is it covered by insurance?
Zynteglo and Casgevy carry list prices in the United States of approximately $2.8 million per treatment. Coverage varies widely by insurer and country. Some manufacturers offer outcomes-based payment arrangements. Most patients require prior authorization and appeals processes to access coverage.
7. Can gene therapy be used for alpha thalassemia as well?
Current approved therapies target beta thalassemia. Research into gene therapy for alpha thalassemia is ongoing but at an earlier stage, partly because alpha thalassemia involves four genes rather than two, making correction more complex.
8. How does CRISPR-based gene editing for thalassemia differ from lentiviral approaches?
Lentiviral gene therapy adds a functional copy of the beta-globin gene to the patient’s genome. CRISPR-based therapy (Casgevy) edits an existing gene—BCL11A—to reactivate fetal hemoglobin production. Both approaches achieve hemoglobin correction but through different mechanisms, with different safety and manufacturing profiles.
9. How long does the gene therapy process take from start to finish?
The full process typically spans several months. It includes stem cell mobilization and collection, laboratory processing of cells (which can take weeks), conditioning chemotherapy, cell reinfusion, and a hospital recovery period. Patients are monitored closely for months afterward before engraftment is confirmed.
10. Are there advanced thalassemia treatment options available for patients who cannot access gene therapy?
Yes. Luspatercept (Reblozyl) is an FDA-approved therapy that reduces transfusion burden without gene modification. Optimized iron chelation regimens, emerging fetal hemoglobin inducers, and coordinated holistic care plans can significantly improve quality of life for patients who are not candidates for or cannot access gene therapy.







{kind=link}