


Heart complications thalassemia patients face arise from iron overload and chronic anemia, causing cardiomyopathy, arrhythmias, and pulmonary hypertension—largely preventable with early MRI screening and consistent iron chelation therapy.
 Thalassemia is an inherited blood disorder that disrupts hemoglobin production, leading to chronic anemia. The connection between thalassemia and heart health comes down to two main forces: iron overload and the strain of long-term anemia. Together, they make iron overload heart disease in thalassemia one of the most important issues in long-term care.
Thalassemia is an inherited blood disorder that disrupts hemoglobin production, leading to chronic anemia. The connection between thalassemia and heart health comes down to two main forces: iron overload and the strain of long-term anemia. Together, they make iron overload heart disease in thalassemia one of the most important issues in long-term care.
How does iron overload damage the heart?
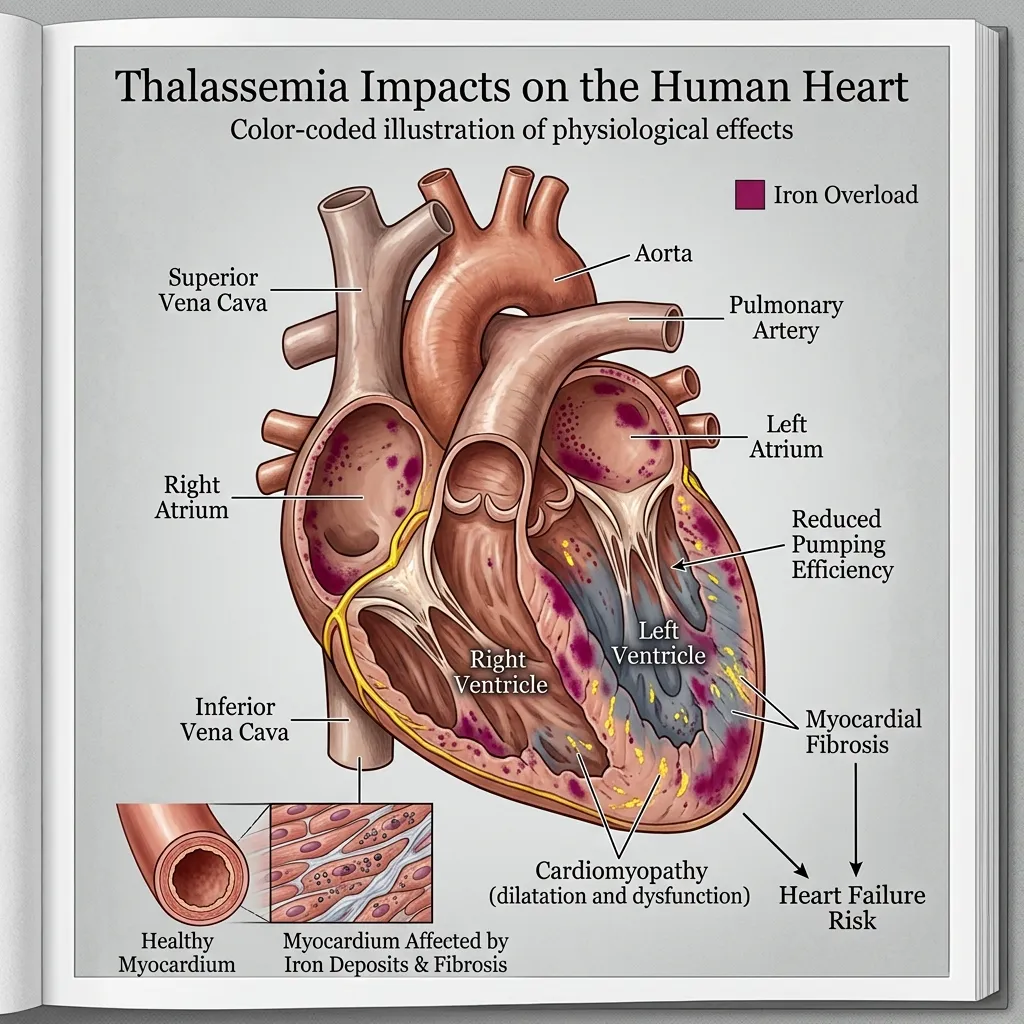
Iron overload is the primary cause of heart complications thalassemia patients experience. The body has no natural way to remove excess iron. Each unit of transfused blood adds roughly 200 to 250 milligrams of iron, and patients with severe beta thalassemia may receive transfusions every two to four weeks. Over months and years, that iron accumulates in organs—including the heart.
Inside cardiac cells, free iron triggers the production of harmful molecules called reactive oxygen species. These molecules damage cell membranes, proteins, and DNA. The result is inflammation, scarring, and weakened heart muscle. Because the heart pumps continuously, even small amounts of iron-related damage can compound over time.
How does chronic anemia strain the heart?
Anemia forces the heart to work harder. When blood carries less oxygen, the heart compensates by pumping faster and harder to meet the body’s needs. This sustained effort can enlarge the heart and, over time, lead to high-output cardiac failure—a state where the heart simply cannot keep up with demand.
In poorly transfused patients, this strain becomes chronic. The combination of low oxygen delivery and constant overwork gradually wears down the cardiac muscle, setting the stage for heart failure.
What other factors contribute to cardiac risk?
Iron overload and anemia are the main culprits, but they are not alone. Iron damages the endocrine glands too, causing hormone imbalances that affect heart function. Chronic inflammation, common in thalassemia, also contributes to vascular and cardiac stress. These factors often overlap, which is why a coordinated care plan matters so much. Our guide on organ damage in thalassemia explores how iron affects the body beyond the heart.
What are the specific heart complications of thalassemia?
Cardiac complications of thalassemia take several forms. Some develop slowly and silently, while others appear suddenly. Knowing each one helps patients and families recognize warning signs early.
What is iron overload cardiomyopathy?
Iron overload cardiomyopathy is the most serious of the heart complications thalassemia patients face. It occurs when iron accumulates in the heart muscle, weakening its ability to pump blood effectively. For decades, this condition was the leading cause of death in patients with beta thalassemia major.
Early on, the disease is often silent. As it progresses, symptoms include shortness of breath, fatigue, swelling in the legs, palpitations, and reduced exercise tolerance. Doctors diagnose it through imaging and cardiac function tests.
The encouraging news is that iron overload heart disease in thalassemia is often reversible when caught early. Intensive iron chelation therapy can remove iron from the heart and restore function—provided treatment begins before permanent scarring sets in. Prognosis depends heavily on how soon the iron burden is identified and addressed.
What arrhythmias and conduction problems can occur?
Iron deposits disrupt the heart’s electrical system, leading to arrhythmias—irregular heartbeats. Common types include atrial fibrillation, premature beats, and conduction abnormalities that slow or block electrical signals.
Symptoms range from harmless palpitations to dizziness, fainting, and, in severe cases, life-threatening rhythm disturbances. Risk rises with the degree of iron loading. Management focuses on lowering iron through chelation, treating the arrhythmia directly with medication, and, in select cases, using a pacemaker to maintain a steady rhythm.
How does pulmonary hypertension develop?
Pulmonary hypertension is high blood pressure in the arteries that supply the lungs. In thalassemia, chronic anemia, abnormal red blood cells, and changes in blood vessel function all contribute. It appears more often in patients who are not regularly transfused.
This condition forces the right side of the heart to work harder, which can eventually lead to right-sided heart failure. Symptoms include breathlessness, fatigue, and chest discomfort, especially during exertion. Doctors typically screen for it using echocardiography, with confirmation through specialized testing when needed.
What about pericardial disease and blood clots?
Two additional complications deserve attention. Pericardial disease involves inflammation of the sac surrounding the heart, which can cause chest pain and, in some cases, fluid buildup. Thromboembolic events—blood clots—are also more common in thalassemia, particularly in patients who have had their spleen removed. These clots can travel to the lungs or brain, making prevention and monitoring important parts of care.
How are cardiac complications of thalassemia diagnosed?
 Early diagnosis is the single most important factor in preventing serious heart damage. Because iron overload cardiomyopathy can stay silent for years, regular screening is essential—even when a patient feels perfectly well.
Early diagnosis is the single most important factor in preventing serious heart damage. Because iron overload cardiomyopathy can stay silent for years, regular screening is essential—even when a patient feels perfectly well.
Why is regular cardiac screening so important?
Heart damage from iron often begins long before symptoms appear. By the time a patient notices breathlessness or swelling, significant damage may already exist. Routine screening catches problems while they are still reversible. This is why consistent monitoring forms the backbone of modern thalassemia care. Our article on why regular checkups matter for thalassemia patients explains how scheduled testing protects long-term health.
What diagnostic tools do doctors use?
Doctors rely on several complementary tests to assess heart health:
- T2 MRI:* This specialized cardiac MRI is the gold standard for measuring iron in the heart. A T2* value below 20 milliseconds signals significant iron loading, allowing doctors to intervene before damage becomes permanent. This single test revolutionized cardiac care in thalassemia.
- Echocardiography: An ultrasound of the heart that shows how well it pumps and screens for pulmonary hypertension and structural changes.
- Electrocardiography (ECG): A quick test that detects arrhythmias and conduction abnormalities.
- Biomarkers: Blood tests such as ferritin estimate overall iron burden, while NT-proBNP can flag early heart strain.
For a deeper look at tracking iron, our guide to iron level monitoring tests breaks down each method in detail.
Who manages cardiac care in thalassemia?
The best outcomes come from a multidisciplinary team. Hematologists, cardiologists, endocrinologists, and specialized nurses work together to monitor iron levels, adjust treatment, and respond quickly to early warning signs. This coordinated approach ensures no single complication slips through the cracks.
How are heart complications in thalassemia treated?
Treating cardiac complications of thalassemia involves two goals: removing excess iron and managing the specific heart problem at hand. When both are addressed together, outcomes improve dramatically.
Why is iron chelation therapy the cornerstone of treatment?
Iron chelation therapy is the foundation of protecting the heart in thalassemia. Chelating agents bind to excess iron so the body can remove it. Three main drugs are used: deferoxamine (infused), deferiprone (oral), and deferasirox (oral). Deferiprone is particularly effective at clearing iron from heart tissue, and combinations are sometimes used for patients with heavy cardiac iron loading.
Adherence matters enormously. Iron overload heart disease in thalassemia develops silently, so patients must stay consistent with chelation even when they feel fine. Early, sustained treatment can prevent cardiomyopathy entirely and reverse it when caught in time.
How do transfusion regimens protect the heart?
Regular transfusions keep hemoglobin at healthy levels, which reduces the strain chronic anemia places on the heart. Well-managed transfusion programs lower the risk of high-output cardiac failure and pulmonary hypertension. The challenge is balance: transfusions ease anemia but add iron, which is precisely why they must be paired with diligent chelation.
How are specific cardiac problems managed?
Beyond iron control, doctors treat individual complications directly:
- Arrhythmias: Managed with antiarrhythmic medications and, when needed, pacemakers or other devices.
- Pulmonary hypertension: Treated with targeted therapies that relax blood vessels and reduce pressure in the lungs.
- Heart failure: Managed with standard heart failure medications to ease symptoms and support cardiac function.
Can emerging therapies cure the underlying problem?
Yes—and this is where the field is changing fastest. Curative treatments target thalassemia at its source, eliminating the need for transfusions and the iron overload that damages the heart. Gene therapies like Casgevy and Zynteglo can free many patients from lifelong transfusions, while stem cell transplants offer a cure for those with a matched donor. Our overviews of emerging treatments for thalassemia and the gene therapy options now available explain how these breakthroughs work and who qualifies.
How can patients prevent heart complications?
 Prevention is far more effective than treatment after damage occurs. A proactive approach can keep the heart healthy for decades.
Prevention is far more effective than treatment after damage occurs. A proactive approach can keep the heart healthy for decades.
What role do early diagnosis and genetic counseling play?
Identifying thalassemia early allows treatment to begin before iron accumulates. Genetic counseling helps families understand inheritance risks and make informed decisions. Together, these steps reduce the chance of severe disease and the cardiac complications that follow.
Which lifestyle choices support heart health?
Patients can protect their hearts with practical habits. Avoiding iron-rich foods and supplements helps limit added iron. Vitamin C in moderation can support chelation, but only under medical guidance. Light to moderate exercise, a balanced diet, and avoiding smoking all benefit cardiovascular health. Patient education is key—understanding why each step matters makes adherence far more likely.
Why does treatment adherence matter so much?
Because iron overload heart disease in thalassemia is silent, the temptation to skip chelation when feeling well is real. But consistent adherence is the single most powerful tool for preventing cardiac damage. Sticking to chelation schedules, attending checkups, and completing regular MRI scans can mean the difference between a healthy heart and irreversible disease.
Living with thalassemia and heart health
Managing a chronic condition takes a toll that goes beyond the physical. The demands of transfusions, daily medication, and regular monitoring can feel overwhelming. Building healthy coping strategies—routines, stress management, and realistic goal-setting—helps patients stay consistent with care.
Support networks make a real difference. Family, friends, fellow patients, and advocacy organizations provide encouragement and practical guidance. Our resources on emotional wellbeing in thalassemia care offer strategies for managing the mental and emotional side of life with a blood disorder. No one should navigate this journey alone.
Conclusion
The story of heart complications thalassemia patients face has changed dramatically. What was once the leading cause of death is now, in most cases, preventable and treatable. The keys are early detection through T2* MRI, consistent iron chelation therapy, well-managed transfusions, and access to a coordinated care team.
For patients today, the outlook is brighter than ever. Curative gene therapies and stem cell transplants now offer the possibility of eliminating the root cause entirely. Trusted organizations like the American Heart Association and the Thalassemia International Federation provide reliable information and support for patients and families.
If you or a loved one is living with thalassemia, talk with your hematologist and cardiologist about a heart-monitoring plan. Stay consistent with chelation, keep your screening appointments, and ask questions. Protecting the heart starts with awareness—and the tools to do it have never been better.
Frequently Asked Questions
1. What are the most common heart complications in thalassemia?
The most common cardiac complications of thalassemia include iron overload cardiomyopathy, arrhythmias, pulmonary hypertension, heart failure, and pericardial disease. Iron overload cardiomyopathy is the most serious and was historically the leading cause of death in thalassemia patients.
2. What causes heart problems in thalassemia patients?
Heart complications thalassemia patients face are caused mainly by iron overload from repeated blood transfusions and by chronic anemia. Excess iron accumulates in heart muscle and damages it, while anemia forces the heart to overwork.
3. Can iron overload heart disease in thalassemia be reversed?
Yes, in many cases. When detected early through T2* MRI, iron overload cardiomyopathy can often be reversed with intensive iron chelation therapy. Reversal becomes far less likely once permanent scarring develops, which is why early monitoring is critical.
4. How is heart iron measured in thalassemia patients?
The gold standard is T2* cardiac MRI, which directly measures iron in the heart muscle. A T2* value below 20 milliseconds indicates significant iron loading. Blood biomarkers like ferritin and NT-proBNP provide additional information.
5. How often should thalassemia patients have heart screening?
Most specialists recommend regular cardiac monitoring, often including an annual T2* MRI for transfusion-dependent patients, along with periodic echocardiography and ECG. Your hematology and cardiology team will set a schedule based on your iron levels and overall health.
6. What are the early warning signs of heart problems in thalassemia?
Early signs include unusual fatigue, shortness of breath, palpitations, reduced exercise tolerance, and swelling in the legs. Because iron overload cardiomyopathy is often silent at first, screening is essential even without symptoms.
7. Does iron chelation therapy protect the heart?
Yes. Iron chelation therapy is the cornerstone of preventing and treating cardiac complications of thalassemia. Drugs like deferiprone, deferasirox, and deferoxamine remove excess iron, and consistent use can prevent or reverse heart damage.
8. Can gene therapy cure heart complications in thalassemia?
Gene therapy and stem cell transplants treat the root cause of thalassemia by reducing or eliminating transfusion dependence. This stops new iron from accumulating, which protects the heart. Existing iron still needs to be managed with chelation.
9. Is pulmonary hypertension common in thalassemia?
Pulmonary hypertension occurs more often in patients who are not regularly transfused, particularly those with thalassemia intermedia. Regular transfusion programs and screening with echocardiography help detect and manage it early.
10. Can people with thalassemia live a normal life with proper heart care?
Yes. With early diagnosis, consistent iron chelation, regular monitoring, and a coordinated care team, many people with thalassemia maintain good heart health and live full, active lives. Access to curative therapies is improving outcomes even further.







{kind=link}