


Iron overload liver damage occurs when excess iron accumulates in liver tissue, triggering oxidative stress, fibrosis, and—if untreated—cirrhosis or liver cancer. The most common causes include hereditary hemochromatosis, beta-thalassemia, and frequent blood transfusions.
Early diagnosis through blood tests and MRI, combined with phlebotomy or iron chelation therapy, can prevent permanent damage.
The liver is the body’s primary iron storage organ. Under normal conditions, it holds iron safely. But when iron accumulates faster than the body can manage—whether due to genetics, disease, or repeated transfusions—the liver pays a steep price. Iron overload liver damage is one of the most serious complications of chronic iron excess, and it develops quietly, often without noticeable symptoms until significant harm has already occurred.
For patients living with conditions like beta-thalassemia or hereditary hemochromatosis, iron overload is not a distant risk—it is a predictable consequence of the disease itself. Transfusion-dependent patients may receive blood every two to four weeks, and each unit deposits roughly 200 to 250 milligrams of iron into their system. Over months and years, that accumulation becomes a medical emergency.
This guide explains how iron overload damages the liver, what symptoms and diagnostic tools to look for, and which treatment strategies—from phlebotomy to iron chelation therapy—offer the best protection. Understanding these mechanisms gives patients, caregivers, and clinicians the foundation they need to act before damage becomes irreversible.
What Is Iron Overload and Why Does It Harm the Liver?
What is iron overload?
Iron overload, also called hemosiderosis or siderosis depending on the context, is a condition in which the body accumulates excess iron beyond its normal storage capacity. The human body has no dedicated mechanism for excreting iron. It regulates iron levels almost entirely through the rate of absorption in the gut—which means any disruption to that regulation can lead to progressive buildup.
Once iron exceeds safe storage limits, it spills into parenchymal cells—the functional cells of organs like the liver, heart, and pancreas. There, it causes direct cellular damage through a process involving reactive oxygen species.
Why is the liver particularly vulnerable to iron overload?
The liver sits at the center of iron metabolism. It produces hepcidin, the hormone that regulates iron absorption across the body. It stores iron in a protein called ferritin and processes transferrin-bound iron delivered by the bloodstream. Because the liver receives iron-rich blood directly from the portal vein, it is the first major organ to bear the burden of excess iron.
Hepatocytes—the main functional cells of the liver—are especially sensitive to iron toxicity. When iron concentrations in liver tissue rise beyond a threshold, the damage cascade begins. According to a review published in the Journal of Hepatology, liver iron concentration above 15 mg/g dry weight is associated with a significantly elevated risk of fibrosis and cirrhosis.
How serious is iron overload liver damage?
Left unaddressed, liver damage from iron overload follows a predictable and serious trajectory: from mild inflammation to fibrosis, then cirrhosis, and ultimately hepatocellular carcinoma—the most common form of primary liver cancer. The risk of hepatocellular carcinoma in patients with cirrhosis from iron overload is estimated to be substantially higher than in the general population, making early intervention critical.
Understanding Iron Metabolism and the Causes of Iron Overload
How does normal iron absorption and storage work?
The body absorbs dietary iron primarily in the duodenum. Hepcidin, produced by the liver, acts as the master regulator—when iron stores are sufficient, hepcidin signals the gut to reduce absorption. When stores are low, absorption increases.
Iron is transported in the blood bound to transferrin and stored in cells as ferritin. The liver stores the largest reserves. This tightly controlled system works well under normal circumstances. When it breaks down—due to genetics, disease, or external factors like transfusions—excess iron accumulates in organs.
What genetic and acquired conditions cause iron overload?
Hereditary Hemochromatosis
Hereditary hemochromatosis is the most common genetic cause of iron overload in populations of Northern European descent. Mutations in the HFE gene (most commonly C282Y and H63D) impair hepcidin regulation, causing the gut to absorb far more iron than the body needs. According to the American College of Gastroenterology, approximately 1 in 200 to 300 people of European ancestry carry the homozygous C282Y mutation. Without treatment, iron accumulates over decades, eventually causing liver damage from iron overload, diabetes, joint disease, and heart complications.
Beta-Thalassemia and Other Anemias
Patients with beta-thalassemia major require blood transfusions every two to four weeks for survival. Each transfusion introduces iron that the body cannot excrete, making transfusional iron overload the primary driver of organ damage in this population. For a detailed look at how thalassemia affects other organs, see our guide on organ damage in thalassemia.
Other anemias, including sideroblastic anemia and myelodysplastic syndromes, carry similar risks when patients depend on long-term transfusions.
Frequent Blood Transfusions
Even in patients without an underlying anemia disorder, repeated blood transfusions—such as those given during cancer treatment—can cause iron accumulation. Each unit of packed red blood cells contains approximately 200 to 250 mg of iron, and the body has no natural pathway to eliminate it.
Dietary Factors and Supplements
High dietary iron intake or excessive supplementation rarely causes severe iron overload on its own. However, in individuals with subclinical genetic variants affecting iron regulation, combined dietary and genetic factors can push iron stores into a dangerous range. Alcohol consumption compounds the risk by directly damaging the liver and impairing its ability to manage iron safely.
The Pathophysiology of Iron Overload Liver Damage
How does excess iron harm liver cells (hepatocytes)?
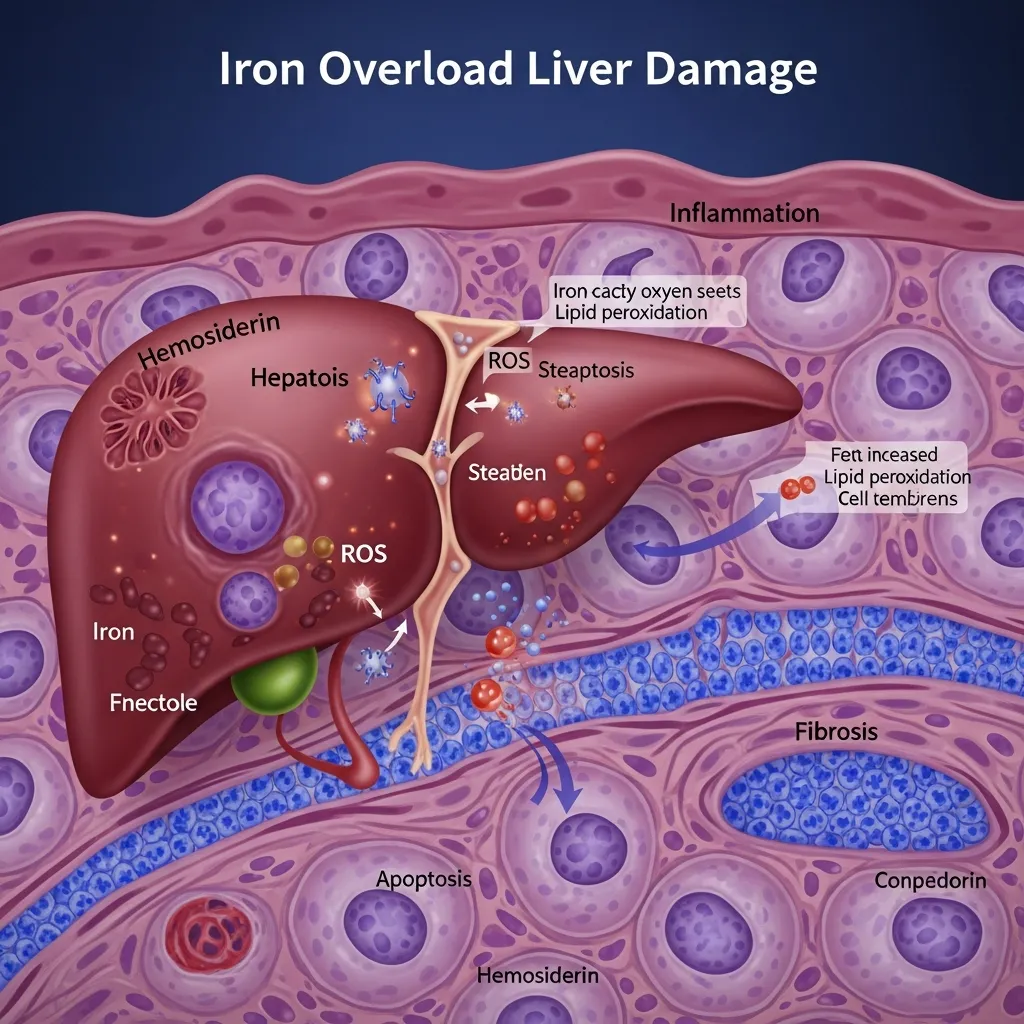
Oxidative Stress and Free Radical Formation
When iron accumulates inside hepatocytes in its unbound, labile form, it participates in the Fenton reaction—a chemical process that converts hydrogen peroxide into highly reactive hydroxyl radicals. These free radicals attack cell membranes, proteins, and DNA indiscriminately, causing widespread cellular damage. This oxidative stress is the primary mechanism behind iron overload liver damage at the cellular level.
Lipid Peroxidation and Mitochondrial Dysfunction
Free radicals trigger lipid peroxidation, which destroys the fatty acid components of cell membranes. As mitochondrial membranes are damaged, energy production inside hepatocytes collapses. Cells lose the ability to carry out basic metabolic functions. Over time, this dysfunction leads to hepatocyte death and triggers inflammatory signaling pathways.
Activation of Hepatic Stellate Cells and Fibrosis
Dead and damaged hepatocytes release signals that activate hepatic stellate cells—the liver’s resident scar-forming cells. Once activated, these cells produce excess collagen, which builds up as fibrous tissue within the liver. This fibrosis stiffens the liver structure, disrupts blood flow, and progressively replaces functional tissue. Iron chelation therapy can slow or halt this process when initiated early.
How does iron overload progress from steatosis to cirrhosis and hepatocellular carcinoma?
The progression follows a recognizable pattern. Early iron accumulation causes hepatic steatosis—fat accumulation in liver cells—combined with mild inflammation. As iron burden increases, fibrosis develops, initially around central veins and portal tracts. Bridging fibrosis connects these areas, and when the entire liver architecture becomes scarred and nodular, the condition has progressed to cirrhosis.
Cirrhosis marks a point of substantially increased risk. Patients with cirrhosis from iron overload face a 200-fold higher relative risk of hepatocellular carcinoma compared to individuals with normal liver iron levels, according to data cited by the European Association for the Study of the Liver. Crucially, some research suggests that iron removal through phlebotomy or chelation may reduce—but not eliminate—this cancer risk even after cirrhosis has developed.
Clinical Manifestations and Diagnosis
What are the early symptoms of liver damage from iron overload?
Iron overload complications develop insidiously. Early symptoms are often nonspecific and easy to dismiss: persistent fatigue, mild right-sided abdominal discomfort, or slight swelling in the liver detected during a physical examination. Skin hyperpigmentation—a bronze discoloration sometimes called “bronze diabetes” in hereditary hemochromatosis—may appear. Joint pain is common, particularly in the knuckles of the index and middle fingers.
By the time symptoms become pronounced—severe fatigue, jaundice, ascites, or signs of liver failure—significant damage has already occurred. This silent progression makes screening essential for anyone with known risk factors.
What diagnostic tools confirm iron overload liver damage?
Blood Tests: Ferritin, Transferrin Saturation, and Liver Enzymes
Serum ferritin and transferrin saturation are the standard first-line tests. Transferrin saturation above 45% in women or 50% in men, combined with elevated ferritin, warrants further investigation. Liver enzymes (ALT, AST, GGT) may be mildly elevated in early disease. For a detailed breakdown of monitoring approaches, see our guide to iron level monitoring tests.
Imaging Studies: MRI (T2*), CT Scan, and Ultrasound
MRI using the T2* sequence is the gold standard non-invasive method for quantifying liver iron concentration. A liver T2* value indicating high iron concentration correlates directly with the degree of hepatic iron loading. CT scanning and ultrasound can identify structural changes associated with cirrhosis but are less precise for iron quantification.
Liver Biopsy: Gold Standard for Severity Assessment
Liver biopsy remains the most definitive method for assessing the degree of fibrosis and confirming the diagnosis in ambiguous cases. Tissue samples are evaluated using the Hepatic Iron Index—a calculation of iron concentration adjusted for age—and graded for fibrosis using established scoring systems. Biopsy is typically reserved for cases where non-invasive tests leave significant diagnostic uncertainty.
Management and Treatment Strategies for Iron Overload Liver Damage
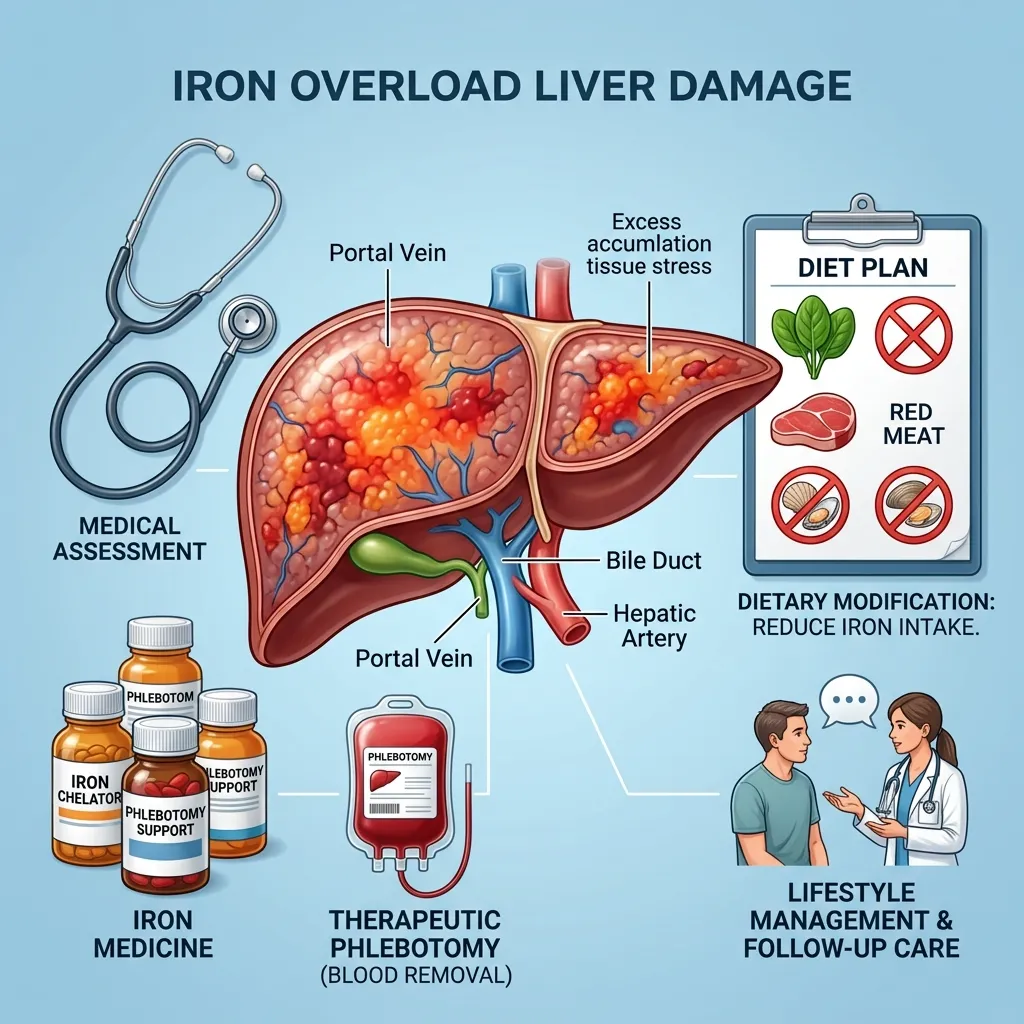
Phlebotomy: The cornerstone of treatment for hereditary hemochromatosis
Therapeutic phlebotomy—the regular removal of blood—is the most effective treatment for hereditary hemochromatosis. Each 450 mL blood donation removes approximately 200 to 250 mg of iron. Initial intensive phlebotomy (often weekly) depletes excess iron stores over six to thirty months, depending on the degree of overload. Maintenance phlebotomy (every two to four months) then sustains normal iron levels long-term.
When started before cirrhosis develops, phlebotomy can normalize liver function and significantly reduce the risk of progression to liver cancer. The treatment is simple, inexpensive, and well-tolerated by most patients.
Iron Chelation Therapy: A lifesaving intervention
For patients who cannot undergo phlebotomy—particularly those with transfusion-dependent thalassemia or other anemias—iron chelation therapy is the primary tool for managing iron overload complications.
Deferoxamine, Deferiprone, and Deferasirox
Three main chelating agents are used in clinical practice:
- Deferoxamine (DFO): The oldest available agent, administered by subcutaneous or intravenous infusion over 8 to 12 hours. Highly effective at reducing liver iron, but the infusion burden reduces adherence.
- Deferiprone (DFP): An oral agent with particular efficacy for cardiac iron. Often combined with deferoxamine for patients with severe multi-organ iron loading. Requires monitoring for agranulocytosis.
- Deferasirox (DFX): Once-daily oral chelation with strong evidence for liver iron reduction. The most widely prescribed agent globally. Requires monitoring for renal and hepatic side effects.
When is chelation therapy indicated?
Iron chelation therapy is indicated when liver iron concentration exceeds safe thresholds, typically above 3 to 7 mg/g dry weight depending on the clinical context, or when serum ferritin rises above 1,000 mcg/L in transfusion-dependent patients. Our overview of thalassemia complications in adults discusses how clinicians weigh these thresholds in long-term management.
Managing side effects and adherence
All three agents carry potential side effects. Adherence is the single greatest predictor of treatment success. Poor adherence allows iron to continue accumulating, negating the protective effect of chelation. Regular counseling, simplifying treatment regimens, and involving multidisciplinary care teams all improve long-term outcomes.
Dietary Modifications to Reduce Iron Absorption
Dietary changes alone cannot reverse iron overload, but they reduce the rate of further accumulation.
Patients should avoid:
- Iron supplements unless specifically prescribed
- High-dose vitamin C (which enhances iron absorption)
- Alcohol, which worsens liver damage and impairs iron regulation
- Raw shellfish, which poses a serious infection risk in patients with liver disease
Tea consumed with meals can modestly reduce dietary iron absorption. Patients should work with a dietitian to build a practical plan that supports overall liver health without unnecessary restriction.
Monitoring and Preventing Further Damage
Ongoing monitoring is non-negotiable. Ferritin and transferrin saturation should be checked regularly—often every three months during active treatment. Annual or biannual liver MRI tracks changes in hepatic iron concentration. Liver function tests, platelet counts, and imaging for cirrhosis complications are adjusted based on disease stage and treatment response.
Preventing and Managing Iron Overload Complications

What other complications develop beyond the liver?
Iron overload complications extend well beyond hepatic disease. Excess iron damages the heart, causing cardiomyopathy and arrhythmias—cardiac iron overload remains a leading cause of death in transfusion-dependent patients. The pancreas suffers too, leading to insulin-dependent diabetes. Endocrine glands including the thyroid, adrenal glands, pituitary, and gonads are all vulnerable, with hypogonadism and growth failure common in younger patients. Our dedicated article on liver iron overload symptoms explores the hepatic presentation in greater detail.
Regular screening and early intervention
The most effective way to prevent severe iron overload liver damage is to identify at-risk patients before damage accumulates. Screening guidelines from major hepatology and hematology organizations recommend:
- Annual ferritin and transferrin saturation in patients with hereditary hemochromatosis or transfusion-dependent conditions
- Liver MRI every one to two years in patients with known elevated iron stores
- Family screening for first-degree relatives of hereditary hemochromatosis patients
Lifestyle adjustments for liver health
Patients with liver damage from iron overload benefit from the same lifestyle measures recommended for any chronic liver disease: maintaining a healthy weight, avoiding alcohol entirely, getting vaccinated against hepatitis A and B, and exercising regularly to support metabolic health. These measures do not remove iron, but they reduce the additional burden placed on a liver already under stress.
Living with Iron Overload and Liver Damage
Patient education and support
Understanding iron overload is the foundation of effective self-management. Patients who know why phlebotomy or chelation is required—and what the consequences of skipping treatment are—adhere better to their care plans. Patient advocacy organizations, including the American Liver Foundation and the Iron Disorders Institute, provide educational resources, support networks, and clinical guidance for individuals and families.
The importance of adherence to treatment
Whether the regimen involves weekly phlebotomy appointments or daily oral chelation, adherence is what separates good outcomes from poor ones. Iron does not stop accumulating during treatment breaks. Even a few months of missed therapy can allow iron to rebuild in liver tissue, reversing hard-won progress. Patients who struggle with adherence should discuss barriers openly with their care team—dose adjustments, alternative agents, and practical support can all help.
Prognosis and long-term management
Patients who begin treatment before cirrhosis develops have an excellent prognosis. Liver function can normalize, fibrosis can stabilize or partially reverse, and life expectancy approaches that of the general population. Once cirrhosis is established, the outlook becomes more guarded—iron removal may slow further progression but cannot undo existing scar tissue. These patients require regular screening for hepatocellular carcinoma, typically with ultrasound every six months.
For patients with thalassemia, emerging curative therapies are transforming the long-term picture. Gene therapy options such as Casgevy and Zynteglo can eliminate transfusion dependence, stopping new iron accumulation at its source. Our guide to emerging treatments for thalassemia covers what these advances mean for patients at risk of iron-related organ damage.
Conclusion
Iron overload liver damage is serious, progressive, and—critically—preventable. The tools to identify it early are widely available. The treatments, whether phlebotomy or iron chelation therapy, are proven effective. What makes the difference between a patient who develops cirrhosis and one who maintains a healthy liver for decades is almost entirely a matter of how early the problem is found and how consistently it is treated.
If you or a loved one has a condition that raises the risk of iron overload—hereditary hemochromatosis, thalassemia, or a history of frequent transfusions—speak with a hepatologist or hematologist about a monitoring plan. Review iron levels regularly. Understand the symptoms that warrant prompt attention. And adhere to treatment, even when you feel well.
Iron overload does its damage quietly. The response needs to be consistent and proactive.
Frequently Asked Questions
1. What is iron overload liver damage, and how does it occur?
Iron overload liver damage occurs when excess iron accumulates in liver cells (hepatocytes), generating free radicals that damage cell structures, trigger inflammation, activate scar-forming cells, and ultimately cause fibrosis and cirrhosis. The liver is the primary iron storage organ, making it the first and most severely affected by iron excess.
2. What are the most common causes of iron overload?
The most common causes include hereditary hemochromatosis (a genetic condition affecting iron absorption), transfusion-dependent anemias such as beta-thalassemia, and frequent blood transfusions for any medical reason. Less commonly, excessive dietary iron intake combined with genetic susceptibility can contribute.
3. What are the early warning signs of liver damage from iron overload?
Early signs are often vague: persistent fatigue, mild right-sided abdominal discomfort, elevated liver enzymes on blood tests, and bronze or gray skin discoloration. Many patients have no symptoms at all in the early stages, which is why screening is essential for those with known risk factors.
4. How is iron overload liver damage diagnosed?
Diagnosis typically begins with blood tests measuring serum ferritin and transferrin saturation. Elevated values prompt liver MRI (using T2* sequences) to quantify hepatic iron concentration. In ambiguous cases, liver biopsy provides definitive assessment of iron level and fibrosis severity.
5. What is iron chelation therapy, and when is it used?
Iron chelation therapy uses medications—deferoxamine, deferiprone, or deferasirox—to bind excess iron and allow the body to excrete it. It is used primarily in patients who cannot undergo phlebotomy, such as those with transfusion-dependent thalassemia. Chelation is indicated when liver iron concentrations or serum ferritin exceed safe thresholds.
6. Is phlebotomy effective for treating iron overload liver damage?
Yes. Therapeutic phlebotomy is the cornerstone of treatment for hereditary hemochromatosis. Regular blood removal depletes iron stores over months to years and can normalize liver function when started before cirrhosis develops. Each 450 mL session removes approximately 200 to 250 mg of iron.
7. Can iron overload liver damage be reversed?
Damage detected before cirrhosis develops can be substantially reversed with consistent iron removal. Fibrosis can stabilize or partially regress, and liver function often normalizes. Established cirrhosis cannot be fully reversed, though treatment can halt further progression and reduce cancer risk.
8. What complications arise if iron overload liver damage goes untreated?
Untreated iron overload progresses from inflammation and fibrosis to cirrhosis, and ultimately to hepatocellular carcinoma. Beyond the liver, iron also damages the heart, pancreas, and endocrine glands, causing cardiomyopathy, diabetes, hypogonadism, and growth failure.
9. How often should patients with iron overload have their liver monitored?
Monitoring frequency depends on disease severity and treatment status. During active treatment, ferritin and liver enzymes are typically checked every three months. Liver MRI is performed annually or biannually. Patients with cirrhosis require ultrasound screening for liver cancer every six months.
10. Are there dietary changes that help manage iron overload?
Diet cannot replace phlebotomy or chelation, but it can reduce the rate of additional iron accumulation. Patients should avoid iron supplements, high-dose vitamin C, alcohol, and raw shellfish. Limiting red meat and eating tea with meals may modestly reduce dietary iron absorption. A dietitian can help build a practical plan.







{kind=link}